The CAMHS Learning Disability (LD) team is a community based specialist service offering support to children and young people, aged between 0 to 18 years, who are experiencing significant mental health problems and who are diagnosed with moderate to severe learning disability.
Jump to read more information on:
- The referral 'journey'
- Communication
- Relationships
- Anxiety
- Sensory Processing
- Stamp Stomp medication pledge
- Additional information for parents and carers
- Frequently asked questions
If you would like to print certain sections of this page, but don't know how, please follow these instructions:
- Highlight the section you want to print.
- Right click, and press the print button.
- You can change your settings to either landscape or portrait, whichever you prefer. Print as you usually would.
- If you would like to view this in a different language, please use the accessibility tool at the bottom of your screen.
Our Team
Our friendly team is made up of:
- Team Coordinator
- Consultant Psychiatrist
- Medical Secretaries
- Clinical Lead/Independent Prescriber/ LD Nurses
- Highly Specialised Clinical Psychologist
- LD Practitioners/ Nurses
- Assistant Practitioners
- Occupational Therapist
- Social Workers
We also offer placements to other professionals, e.g. Trainee Nurse Associates and Trainee Clinical Psychologists.
The referral 'journey'
Referral
Once we receive the referral, one of our qualified clinicians will consider the mental health needs of the child to determine if the CAMHS LD team are the most appropriate service. We may contact you for more information to help make this decision. If we do not feel we are the most appropriate service we may signpost you to other services or support.
Appointment offer
An Initial Assessment appointment will be offered as appropriate; either ‘face-to-face’ or ‘virtually’ (MS Teams). This will depend on your individual needs. One of the medical secretaries will discuss this with the family, prior to the assessment appointment being made.
Initial Assessment
We will then complete the assessment with the parent/ carer; at this stage the child/ young person does not have to be present. We will discuss the child/ young person's emotional wellbeing journey, how they are presenting now and families expectations from the referral.
If appropriate, we will then complete observations of the child/ young person in various settings e.g., home, school, respite, community.
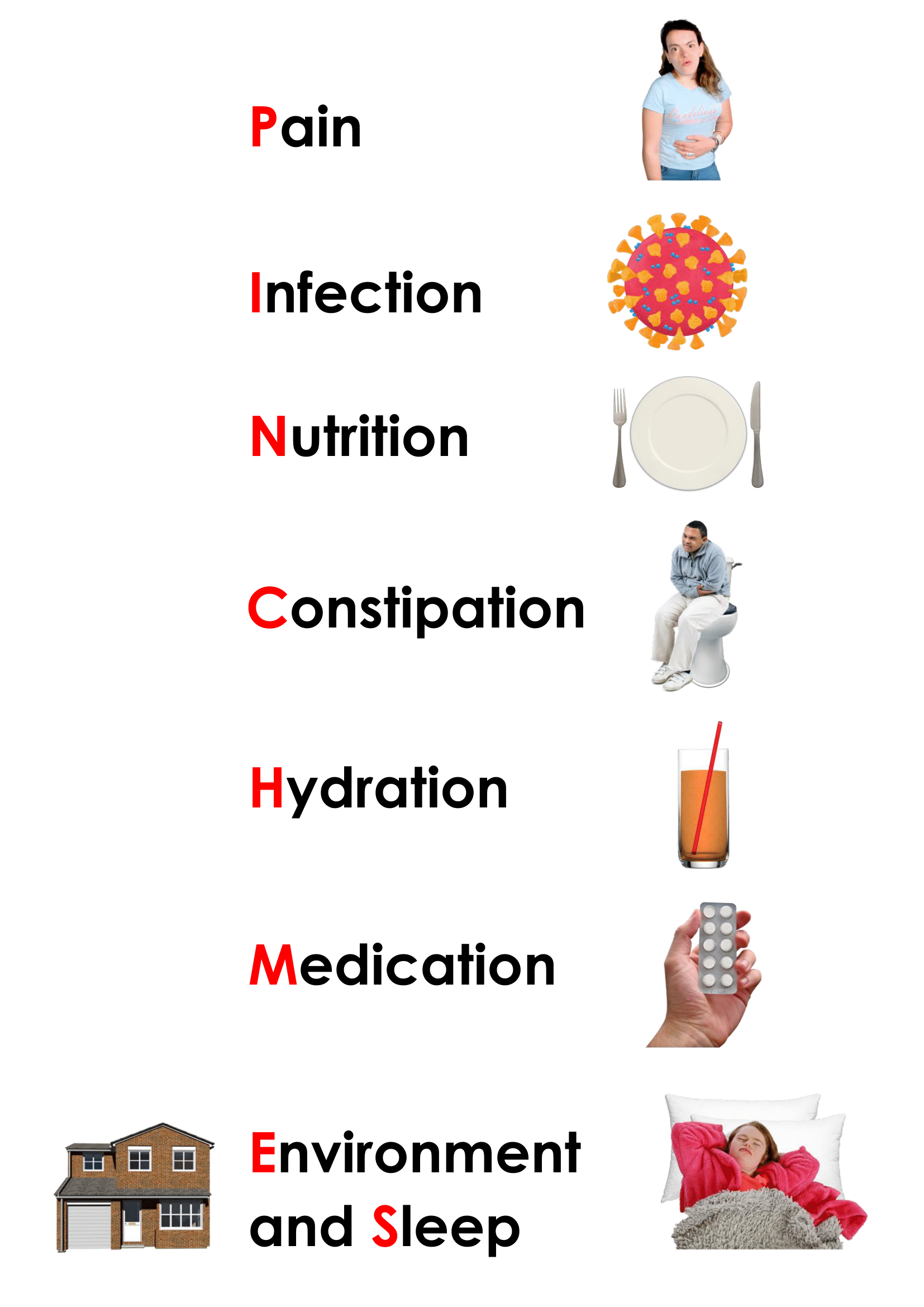
If somebody’s mental health declines, the underlying cause might be that they are physically unwell.
Please consider the PINCHME acronym as a starting point of things to consider that could be impacting on their emotional wellbeing.
We will then discuss the referral as a whole team and decide what interventions we might be able to offer; or we will signpost to other services.
How we can help
The team will work directly with the young person, parents and carers, schools, other health professionals and social care to offer individual tailored advice and strategies to support the young person. This might include:
- Conducting a comprehensive mental health assessment that includes psychological, emotional and behavioural presentation, as well as looking at physical issues which could be affecting a young person's presentation. This could also include mental health medication consultation and review if deemed appropriate.
- Offering individualised mental health treatments and interventions
- Providing consultation and support to other agencies who support our young people and families such as schools, respite services, children’s homes.
- Providing opportunities for parents to access individualised peer support and share experiences in a group setting supported by the CAMHS LD team.
- Signposting to other appropriate agencies
-
We can provide information and support about transitions between services, including the transition to adult services.
This is not an exhaustive list and any intervention would be individualised to the needs of the young person and family.

Communication
Communication is a means of sending and receiving information and comes in many forms. Communication might be through behaviour, physical gesture, or language. Effective and inclusive communication is about having a range of ways to tell people things from simple language to additional tools, techniques, and technologies. Misunderstanding communication can create frustration and can lead to young people using inappropriate ways to ensure their needs are met e.g. through their behaviour.
Anxiety
Anxiety is a natural emotional, psychological and physical response to a perceived threat, this can be due to things happening in the environment, (e.g. a new situation, perceived danger, significant events) or internal triggers (a feeling or a thought). It is there to protect us from harm and to keep us safe (e.g. fight / flight / freeze / fawn response). Sometimes young people may not know why they feel anxious.
Stamp Stomp medication pledge
We are proud to have signed a national Stamp-Stomp medication pledge, to state that we will always aim to prescribe the least amount of the most appropriate medication for the shortest time necessary. This is to provide a ‘window of opportunity’, to support a young person with other therapies or strategies to help their mood, behaviour and emotional regulation.
Medication may be something that is considered by the Teams Consultant Child and Adolescent Psychiatrist or the Independent Prescriber following a holistic assessment of needs and psychological formulation by the whole team. We will discuss our thoughts on the use of medication with you in full, share information leaflets (in easy-read format too if relevant), carefully considering the rationale for a medications use and give you time to think and ask questions of your own before providing consent. This is a very thorough approach, knowing that historically, medication in Learning Disability and autistic populations, have been overused in the past, often with long-term side-effects to physical health and as a form of a restrictive practice.
Additional information for parents and carers
Growing Up, Gaining Independence: information for families of young people with a Learning Disability
The following information was originally produced by Great Ormond Street Hospital for Children NHS Foundation Trust (GOSH).
At LPFT we encourage and support young people to become as independent with their healthcare as they can be. Some people might always need someone else to help them manage their healthcare and to make health-related decisions for them. How these decisions are made and who can make them changes as people get older.
The information below provides detail for families about decision-making when their child is unable to make decisions for themselves once they are 16. While your child is under 18 years old you may hold Parental Responsibility for them. Anyone with Parental Responsibility can manage decisions on their child's behalf, although certain aspects of this change when your child reaches 16 years old.
Gillick competence
The following information was originally produced by the NSPCC (https://learning.nspcc.org.uk/child-protection-system/gillick-competence-fraser-guidelines#skip-to-content - last visited 3 February 2023).
Gillick competency applies mainly to medical advice but it is also used by practitioners in other settings. For example, if a child or young person:
- would like to have therapeutic support but doesn't want their parents or carers to know about it is seeking confidential support for substance misuse
- has strong wishes about their future living arrangements which may conflict with their parents' or carers' views.
Medical professionals need to consider Gillick competency if a young person under the age of 16 wishes to receive treatment without their parents' or carers' consent or, in some cases, knowledge.
If the young person has informed their parents of the treatment they wish to receive but their parents do not agree with their decision, treatment can still proceed if the child has been assessed as Gillick competent.
There is specific guidance for medical professionals on using Gillick competence - see case history and legislation.

